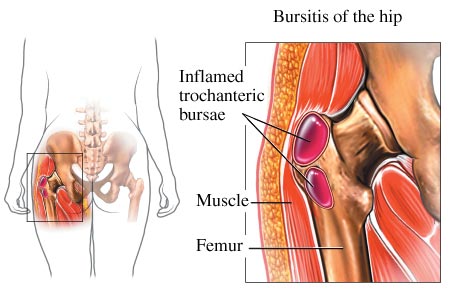
Trochanteric (hip) bursitis or "greater trochanteric pain syndrome”
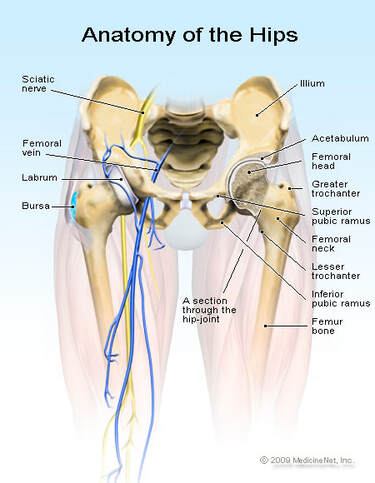
The greater trochanter is a projection in the upper head of the thighbone, near the hip joint, and is the site of attachment for five muscles. Around these bony protrusions and surrounding soft tissues are fluid-filled sacs called bursae which provide cushioning.
Trochanteric bursitis is a common condition of the hips that leads to pain in the outer hip, thigh, and buttocks. It’s a relatively common condition.
Trochanteric bursitis is a common condition of the hips that leads to pain in the outer hip, thigh, and buttocks. It’s a relatively common condition.
The syndrome encompasses a wide range of causes, including muscle tears, tendinosis (chronic degeneration of tendons without inflammation) and other disorders.
It is typically present in middle aged adults, but its frequency in young adults is on the rise, particularly runners. It is four times more frequent in women than in men in the general middle age population. |
|
Symptoms of trochanteric bursitis include:
Common risk factors of trochanteric bursitis:
Diagnosis for trochanteric bursitis:
This is usually clinical, but can be complemented by the use of imaging techniques, especially when making differential diagnosis (that is, considering the possibility that the present symptoms may be due to a different injury).
A thorough history is important and may reveal activities that causes overuse injuries.
The patient usually presents pain in the lateral hip, and tenderness at the greater trochanter when palpated. There is also pain at the extreme of hip rotation, adduction or abduction.
Pain can extend down the outer side of the buttocks and down the outer side of the thighs, but usually not beyond the upper thigh. This feature can be used to differentiate between cases of trochanteric bursitis and other pathologies such as ITB disorders that usually causes pain below the knee.
Imaging techniques such as plain radiographs, ultrasounds, and MRI can greatly assist in making the correct diagnosis.
Treatment
Initial treatment usually involves non-steroidal antiinflammatory drugs (NSAIDs), ice, rest and activity modification.
Patient may also be advised to sleep with a pillow between the knees to minimize bursae compression.
Once the pain decreases, massage can also be introduced to aid in rehabilitation.
Weight loss and physiotherapy to assit in the treatment regimens.
Back, hip, lower limb, foot adjustments can be beneficial to restore full range of motion and biomechanics.
Strengthening muscle imbalances, which may have contributed to the condition is necessary to properly fix biomechanical faults.
Orthotics for the feet and lower limb may be utilized to correct poor foot biomechanics and lower limb discrepancy.
If symptoms are unresponsive, shockwave therapy (ESWT), corticosteroidal injections or local anaesthetics may be given.
If symptoms persist, surgery is considered. Surgical intervention has shown significant success for these patients, and has several options.
- Pain at the hip joint – Pain may be sharp at first, and then dull as time passes. The pain may be aggravated when sitting or lying down for a prolonged period of time, walking up a flight of stairs, sleeping on the affected side, running and climbing
- Difficulty walking
- Joint stiffness
- Joint swelling
- Warmth at the affected site
- A catching and clicking sensation
Common risk factors of trochanteric bursitis:
- Repetitive stress applied to the hip area, for example from running.
- Leg length discrepancy
- Infection and diseases that cause inflammation of the bursae
Diagnosis for trochanteric bursitis:
This is usually clinical, but can be complemented by the use of imaging techniques, especially when making differential diagnosis (that is, considering the possibility that the present symptoms may be due to a different injury).
A thorough history is important and may reveal activities that causes overuse injuries.
The patient usually presents pain in the lateral hip, and tenderness at the greater trochanter when palpated. There is also pain at the extreme of hip rotation, adduction or abduction.
Pain can extend down the outer side of the buttocks and down the outer side of the thighs, but usually not beyond the upper thigh. This feature can be used to differentiate between cases of trochanteric bursitis and other pathologies such as ITB disorders that usually causes pain below the knee.
Imaging techniques such as plain radiographs, ultrasounds, and MRI can greatly assist in making the correct diagnosis.
Treatment
Initial treatment usually involves non-steroidal antiinflammatory drugs (NSAIDs), ice, rest and activity modification.
Patient may also be advised to sleep with a pillow between the knees to minimize bursae compression.
Once the pain decreases, massage can also be introduced to aid in rehabilitation.
Weight loss and physiotherapy to assit in the treatment regimens.
Back, hip, lower limb, foot adjustments can be beneficial to restore full range of motion and biomechanics.
Strengthening muscle imbalances, which may have contributed to the condition is necessary to properly fix biomechanical faults.
Orthotics for the feet and lower limb may be utilized to correct poor foot biomechanics and lower limb discrepancy.
If symptoms are unresponsive, shockwave therapy (ESWT), corticosteroidal injections or local anaesthetics may be given.
If symptoms persist, surgery is considered. Surgical intervention has shown significant success for these patients, and has several options.