Iiotibial band syndrome (ITB)
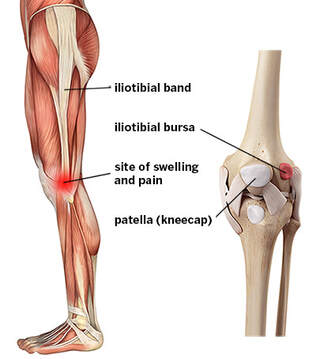
The iliotibial band is a thick tendon located in the outer leg, extending from the top of the hip bone to just below the knee.
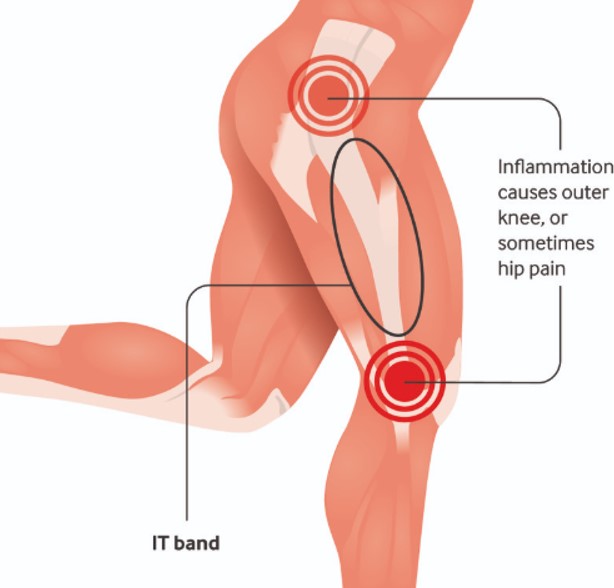
Iliotibial band (ITB) syndrome is a source of knee pain, resulting from inflammation of the lower portions of the iliotibial band. Occasionally, inflammation can occur at the upper end of the iliotibial band, resulting in hip pain.
It is caused by repetitive sliding of the band over the knee that leads to excessive friction acting on the band, irritation, and inflammation. This rubbing of the band against underlying structures occurs when the knee is flexed about 20 to 30 degrees.
Iliotibial band (ITB) syndrome is a source of knee pain, resulting from inflammation of the lower portions of the iliotibial band. Occasionally, inflammation can occur at the upper end of the iliotibial band, resulting in hip pain.
It is caused by repetitive sliding of the band over the knee that leads to excessive friction acting on the band, irritation, and inflammation. This rubbing of the band against underlying structures occurs when the knee is flexed about 20 to 30 degrees.
|
|
This is the one of most common sources of 'overuse' knee pain in runners and cyclists. Although it is most commonly seen in these two sports populations, athletes that participate in volleyball, tennis, soccer, skiing, weight lifting, field hockey, rowing and aerobics are also susceptible to the injury.
Risk Factors
The risk factors are:
Symptoms
Common symptoms are:
Diagnosis
ITB syndrome is often diagnosed clinically. A physical examination and thorough history are crucial in making an accurate diagnosis.
ITB syndrome should be considered for patients that do not recall trauma to the knees, take part in activities known to cause overuse injuries and report that rest has not been helpful in alleviating the pain.
Patients usually complain of a pain in the outer knee region with no specific area of tenderness in this region. This pain intensifies during activity as time passes, as the iliotibial band becomes more irritated.
Pain is aggravated by downhill running, lengthening of the stride and sitting for prolonged periods of time with the knees bent.
As for the physical examination, tenderness occurs when the outer knee is touched 2 centimetres above the joint line and when standing with the knees bent at about 30deg.
Strength in the muscle group that allows the knees to bend and straighten, and in the hip abductors should also be assessed as weakness may be an indication of ITB syndrome.
If in doubt, a MRI may be utilized, especially in making a differential diagnosis to exclude other possible pathologies such as meniscal tears. The MRI may show a thickened iliotibial band, and may also reveal that the bursae, (a sac that surrounds soft tissues and bones to provide cushioning), near the band has become inflamed and filled with excess fluid.
Treatment
Usually consists of:
- activity modification
- treatment of the inflammation
- shockwave therapy (EST)
- stretching and strengthening program
- biomechanical abmormality correction
- and finally the gradual return to normal activities.
Runners that have low mileage respond well to a regimen of stretching and anti-inflammatory drugs, but competitive or high-mileage runners need a more comprehensive treatment plan. Once stretching programme can be done without pain, a strengthening programme can be initiated. Return to running should be gradual and only done once stretching regimen can be performed without pain.
For patients that do not respond well to conservative treatment, surgery should be considered.
Risk Factors
The risk factors are:
- Iliotibial band tightness
- Time spend running or walking on the track
- Downhill running
- Weakness in muscles that act on the knees and hips
- Increased landing forces
- Increase internal rotation of the knee
- Low hamstring strength compared to the quadriceps muscles
Symptoms
Common symptoms are:
- Pain in the outer knee, which might radiate downwards or to the front of the knee. Oftentimes, the pain occurs as one performs aggravating activities, but if injury isn’t severe, the pain may stop once activity has ended.
- Popping in the outer knee – as the patient does the activities.
- Swelling at the lower end of the iliotibial band.
Diagnosis
ITB syndrome is often diagnosed clinically. A physical examination and thorough history are crucial in making an accurate diagnosis.
ITB syndrome should be considered for patients that do not recall trauma to the knees, take part in activities known to cause overuse injuries and report that rest has not been helpful in alleviating the pain.
Patients usually complain of a pain in the outer knee region with no specific area of tenderness in this region. This pain intensifies during activity as time passes, as the iliotibial band becomes more irritated.
Pain is aggravated by downhill running, lengthening of the stride and sitting for prolonged periods of time with the knees bent.
As for the physical examination, tenderness occurs when the outer knee is touched 2 centimetres above the joint line and when standing with the knees bent at about 30deg.
Strength in the muscle group that allows the knees to bend and straighten, and in the hip abductors should also be assessed as weakness may be an indication of ITB syndrome.
If in doubt, a MRI may be utilized, especially in making a differential diagnosis to exclude other possible pathologies such as meniscal tears. The MRI may show a thickened iliotibial band, and may also reveal that the bursae, (a sac that surrounds soft tissues and bones to provide cushioning), near the band has become inflamed and filled with excess fluid.
Treatment
Usually consists of:
- activity modification
- treatment of the inflammation
- shockwave therapy (EST)
- stretching and strengthening program
- biomechanical abmormality correction
- and finally the gradual return to normal activities.
Runners that have low mileage respond well to a regimen of stretching and anti-inflammatory drugs, but competitive or high-mileage runners need a more comprehensive treatment plan. Once stretching programme can be done without pain, a strengthening programme can be initiated. Return to running should be gradual and only done once stretching regimen can be performed without pain.
For patients that do not respond well to conservative treatment, surgery should be considered.